 Figure 1 – MRI scan showing suprasellar craniopharyngioma. Reproduced with parental permission (2025)
Figure 1 – MRI scan showing suprasellar craniopharyngioma. Reproduced with parental permission (2025)
Correct Answer: Triphasic response following pituitary surgery
Explanation:
This pattern reflects the classic triphasic response seen after neurosurgical procedures involving the hypothalamic–pituitary region, especially craniopharyngioma resection[1]:
Phase 1: transient DI
Initial damage to AVP-producing neurons leads to transient central DI, causing polyuria and hypernatremia.
Phase 2: SIADH-like symptoms
SIADH-like phase: Damaged neurons release stored AVP uncontrollably, resulting in water retention, hyponatremia, low urine output, and concentrated urine.
Phase 3: permanent DI
If AVP-producing cells are irreversibly damaged, the patient enters chronic central DI, with polyuria, hypo-osmolar urine, and hypernatremia.
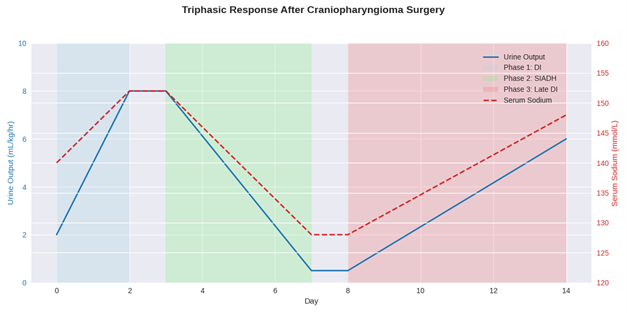
Figure 2 – The triphasic response after craniopharyngioma surgery
Recognising this triphasic pattern is critical for appropriate fluid and endocrine management postoperatively, particularly in the first week following surgery. Strict fluid input and urine output with regular monitoring, or serum sodium and osmolarity paired with urine osmolarity, is key to ensuring that these phases can be identified.
INCREASING WEIGHT GAIN
Despite full pituitary hormone replacement, the 6-year-old girl underwent significant weight gain in the subsequent 6 months, and a rapid and marked increase in her body mass index (BMI) as demonstrated on the BMI chart below [Figure 3]
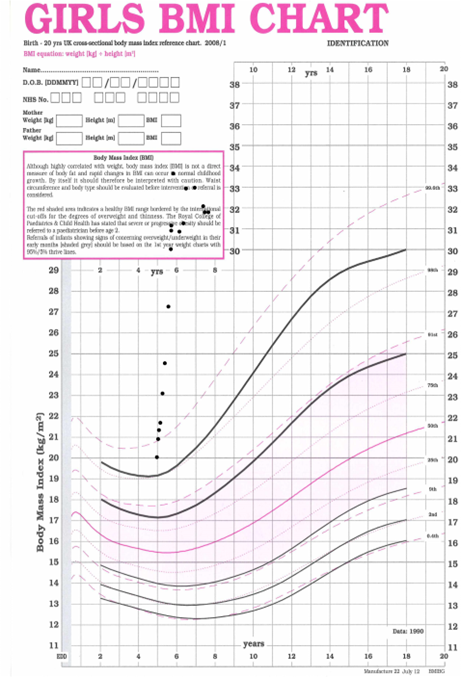
Figure 3. BMI growth chart for craniopharyngioma patient. Generated using Microsoft Copilot 2025.
