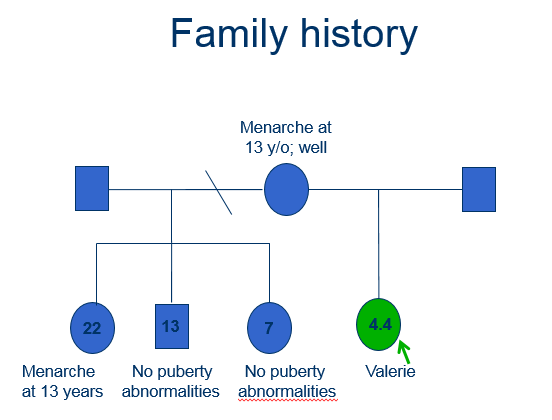
Medical and family history
Female
Age 4.0 years of age
Presented to the Local Paediatric Endocrine clinic
Complaining of:
- Per vagina (PV) bleeding
- 1 episode
- Lasted for 3 days, requiring x 3 sanitary towels a day
- Minimal lower abdominal pain
- Breast development: progressed over the last year
- Axillary and pubic hair development: more recent
Examination
- Well looking
- No café-au-lait spots
- Abdomen slight distension
- suprapubic mass arising from the pelvis
- smooth, mobile, non-tender
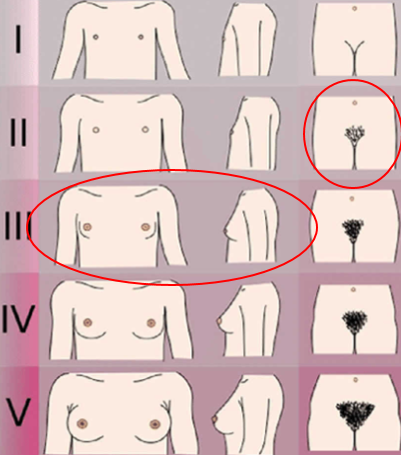
- Pubertal staging (Tanner)
- Breast stage 3 (B3)
- Axillary hair stage 2 (A2)
- Pubic hair stage 2 (P2)
- Vagina appeared oestrogenised
- All other systems unremarkable
Tanner stages of puberty
Along with precocious puberty, you will find café-au-lait spots in a rare condition called McCune-Albright syndrome
McCune-Albright syndrome is a genetic disorder that occurs in both boys and girls, which is characterised by three classic signs:
- Café-au-lait spots
- Bone disorder characterised by symptoms or signs on x-ray
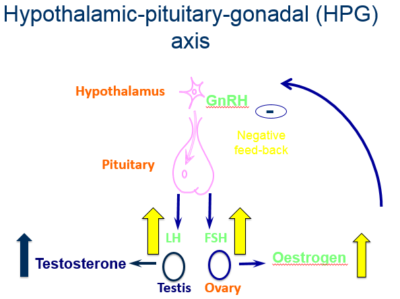
- Endocrine gland hyperfunction; most commonly in girls this hyperfunction involves the ovary, resulting in gonadotrophin- independent precocious puberty

Radiology findings
- Abdominal and pelvic Magnetic Resonance Imaging (MRI) scan
- Scan revealed a large mass approximately 15 cm x 10 cm
